follow up for papillary thyroid cancer
- related: Endocrine
- tags: #endocrine
This patient has a low risk for recurrent thyroid cancer due to young age (< 45 years) and small (< 4 cm) nonmetastatic tumor. Papillary thyroid cancer is the most common type of thyroid cancer and usually recurs in the neck. The prognosis is usually very good in small tumors without high-risk features (eg, vascular invasion, more aggressive histologic subtypes, or poorly differentiated histologies on pathology). Most cancers require initial thyroidectomy and post-surgical radioiodine therapy. Thyroglobulin is secreted by most differentiated thyroid cancers (papillary and follicular) and is a useful marker of persistent or recurrent tumor after thyroidectomy and radioablation of normal thyroid tissue. Undetectable thyroglobulin in treated thyroid cancer patients signifies absent disease.
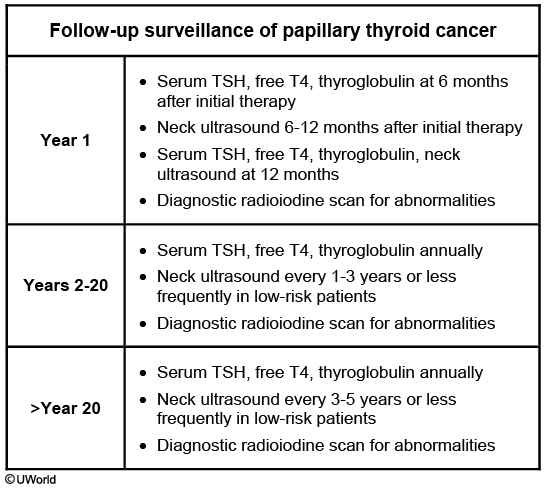
Follow-up surveillance (Table) includes serial TSH, free T4, and thyroglobulin measurements. Neck ultrasound is recommended twice initially in the first year after cancer treatment and then every 1-3 years or less frequently in low-risk patients. Diagnostic radioiodine scan is recommended for elevated thyroglobulin. This patient has been followed for 3 years without evidence of residual thyroid cancer. Her symptoms are nonspecific, and she first needs serum TSH, free T4, and thyroglobulin to assess for recurrent thyroid cancer (Choice C). If thyroglobulin is elevated, she may require further testing, including neck ultrasound and diagnostic radioiodine scan (Choices B and D).